

Una sessualità soddisfacente è un elemento fondamentale della salute fisica e psichica e va tutelata a ogni età. Quando si manifestano disturbi, un sereno dialogo tra i partner e il supporto medico sono la chiave per risolvere la situazione.
Sexuality is not only a source of pleasure, but is a fundamental aspect of the physical and psychological health of every person, man or woman, regardless of age. Recognizing and affirming this for several decades is even the World Health Organization (WHO), which includes sexuality among the cornerstones of the official definition of health.
At every age, however, men and women have a different way of experiencing sexuality and may experience various disorders that can risk turning an extraordinary source of balance and well-being into a problem that is anything but trivial, even to the point of causing them to avoid relationships altogether in order to avoid feeling distressed.
An essential concept to remember, in these cases, is that sexuality is never an individual matter, but a couple’s experience and as such must be dealt with, both when everything is going perfectly and when there is something wrong. Remedies to resolve the situation are many and effective in most cases, but they work best if two people are handling them, with serenity, a spirit of cooperation and mutual affection.
The difficulties of youth
As young people, in the absence of specific pathologies of the genitourinary system or severe systemic diseases, the main critical issues in the sexual sphere are generally related to insecurity and fear of “not being up to par” (because they are not fit enough, sensual or “technically prepared”) or inexperience and a lack of confidence with one’s body, leading to not knowing how to manage one’s emotions and the physical reactions that accompany them.
All these unresolved psychological difficulties can interfere with desire or lead to reaching the climax of pleasure too early, too late, with extreme difficulty or even never. Included in this group of sexuality disorders are: performance anxiety, erectile dysfunction, and premature or delayed ejaculation, on the male side; insufficient desire, unpleasant or painful intercourse, and difficulty reaching orgasm, on the female side.
Problems can occur from the earliest relationships and be particularly difficult to deal with given the limited experience of both partners and, not infrequently, from the precariousness of the relationships. These early critical issues can undermine the quality of one’s later sex life if not addressed early, by talking frankly to one’s partner and/or seeking the support of one’s medical professional and possibly a psychologist experienced in sexuality disorders.
In general, disturbances without an objective organic basis are more frequent and significant during relationships that are short-lived and characterized by a lack of mutual empathy while they greatly improve (until they disappear) when a deep and lasting relationship can be established, which allows one to find a good physical and psychological harmony and to experience sexuality in a gradually more relaxed and natural way.
On the other hand, even young, healthy and initially close-knit couples may, at some point, lose interest in sexual activity or derive less pleasure from it. In these cases, the origin of the problem often has to be sought in factors of a different nature, such as instability or stress at work, worry about economic difficulties, fatigue due to too many commitments, insufficient sleep or unhealthy lifestyle.
In this regard, it should be remembered that smoking, alcohol, being overweight, low physical activity and disordered life rhythm are declared enemies not only of general health, but also of sexual health (especially for men). Their negative impact is felt at every age and becomes gradually more pronounced as we approach “age.”
Another critical phase for couples of childbearing age is that of pregnancy and postpartum, due to a mix of physical and psychological factors that can put a strain on both partners, for different and sometimes opposing reasons, especially at the time of the first child.
Reduced desire, fear of harming the fetus, anxiety about becoming a parent, postpartum physical and psychological discomfort, arrival of the newborn, and redefinition of family balance can seriously interfere with sexuality for several months, especially if it is not discussed within the couple and support from the gynecologist (for the woman) and possibly the psychologist (for both partners) is not sought.
Maturity disorders
Like all functions of the organism, the sexual function also transforms with the passage of time, and although some may be annoyed or disappointed by it, all that remains is to accept the inevitable change, which nonetheless also has some positive implications such as greater experience, more relaxed approach to relationships, finer knowledge of oneself and partner, etc.
In both men and women, what drives the transformation is primarily the gradual decline in sex hormone levels (androgens and estrogens, respectively) that occurs from the age of 40-50, compounded by a progressive decrease in muscle and cardiovascular performance and, in many cases, the onset of diseases or disorders that may interfere with sexuality either directly or as a consequence of the therapies one has to take to keep them under control.
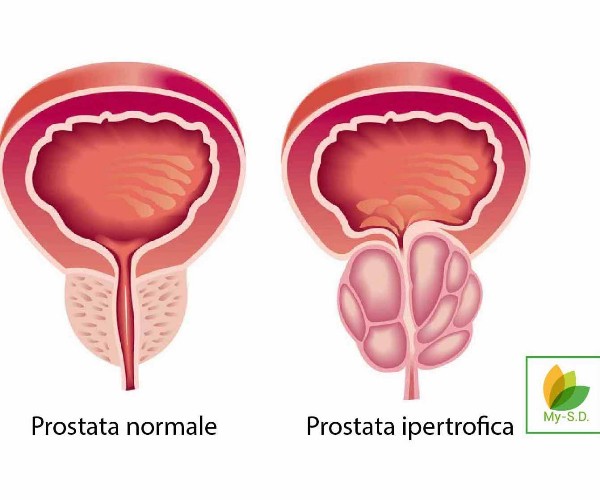
In men, for example, many cardiovascular diseases, type 2 diabetes, and prostatic disorders can reduce the ability to achieve an erection or maintain it, as can medications needed to lower high blood pressure or hyperglycemia, counteract coronary artery disease or symptoms of prostatic hypertrophy, and improve heart function in those with atrial fibrillation or heart failure.
In women to interfere with sexuality can be ovarian, thyroid, or pituitary dysfunction and symptoms associated with menopause or postmenopause, starting with decreased lubrication and gradual changes in vaginal mucosal sensitivity and structure (all changes that can result in unpleasant or painful intercourse).
Also not to be overlooked are the conditions of mental distress that can become particularly prevalent and pronounced in women over 40, first and foremost depression and anxiety (from which men also suffer less frequently), as well as the negative repercussions on sexuality of some of the medications required to treat them (antidepressants, mood stabilizers, etc.). Also on the psychological front, especially when confronted with a new partner, creating problems when one is no longer very young can be the idea of not having an aesthetically desirable body, at least according to current standards: in this case, greater awareness of one’s own value and a little self-deprecation are the keys to success.
How to solve the situation?
Assuming that sexuality is a couple’s issue, the first piece of advice for dealing with any kind of physical or psychological problem is to talk about it openly with your partner(s), simply and calmly. This will also help the partner not to feel like the “cause” of the reduced desire or less pleasure experienced, and will allow the level of intimacy and cohesion of the couple to increase, as well as sometimes to identify together, without too much difficulty, an appropriate solution.
If sharing the problem and addressing it together with simple strategies (e.g., creating more stimulating situations, prolonging foreplay, changing positions, modulating the timing of reaching orgasm, etc.) is not enough to improve the situation, the next step is to contact your medical professional to check your general health status, assess the specific disorder, and identify possible interventions that can help alleviate it (see, for example, erectile dysfunction drugs or hormone therapies).
Seeking medical advice before taking any type of medication or supplement is essential, both because the drugs available to improve sexual performance can have several contraindications and be dangerous in certain clinical settings and because, at times, sexual dysfunction can be a telltale sign of an as-yet undiagnosed organic disease that needs to be evaluated and managed (such as, for example, cardiovascular disease, hormonal disorders, or prostate problems).
When the sexuality disorder appears to be related to genitourinary aspects, a gynecological (for women) or andrological/urological (for men) consultation should be sought. Especially after the age of 50, it is especially at this level that disorders capable of greatly reducing the possibility of having satisfactory relationships (or having them tout-court) can arise, and it is important that an experienced specialist be the one to investigate the causes and suggest appropriate solutions, whether pharmacological or surgical.
Sources:
- National Institute on Aging – NIH (https://order.nia.nih.gov/publication/sexuality-in-later-life)
- Mayo Clinic (https://www.mayoclinic.org/diseases-conditions/female-sexual-dysfunction/symptoms-causes/syc-20372549)
- Mayo Clinic (https://www.mayoclinic.org/diseases-conditions/erectile-dysfunction/symptoms-causes/syc-20355776)
- Mayo Clinic (https://www.mayoclinic.org/diseases-conditions/premature-ejaculation/symptoms-causes/syc-20354900)
- Mayo Clinic (https://www.mayoclinic.org/diseases-conditions/delayed-ejaculation/symptoms-causes/syc-20371358)
- von Hippel C et al. Sexual Function among Women in Midlife: Findings from the Nurses’ Health Study II. Women’s Health 2019;29-4:291-298
- Hatzichristou D et al. Clinical Evaluation and Management Strategy for Sexual Dysfunction in Men and Women. Journal of Sexual Medicine 2004;1(1):49-57
- Knoepp LR et al. Sexual Complaints, Pelvic Floor Symptoms, and Sexual Distress in Women over Forty. Sex Med 2010;7:3675-3682
- Avasthi A et al. Clinical Practice Guidelines for Management of Sexual Dysfunction. Clinical Practice Guidelines for Management of Sexual Dysfunction. Indian J Psychiatry 2017;59(Suppl 1):S91-S115
- Mernone L et al. Psychobiological Factors of Sexual Functioning in Aging Women – Findings From the Women 40+ Healthy Aging Study. Frontiers in Psychology 2019;10:546