Anxiety has a thousand faces, and the ways in which it manifests itself can change over time, with varying pervasiveness and severity.
Diagnosis is essentially based on two basic concepts: the specific centrality of the disorder and its clinical significance.
That is, the clinician must ask: What causes the patient to seek help from the physician? What are the central symptoms (psychopathological core) that cause suffering? What is the main characteristic of these symptoms and in what category of disorders can they be recognized? Do the symptoms have clinical significance? That is, do they cause “clinically significant impairment or discomfort?
Anxiety can manifest itself
- In acute form, such as panic attack
- Or sneaky, unpleasant and aggravating, such as generalized anxiety
Symptomatology may appear suddenly, in the midst of mental and physical well-being, out of the blue, with no apparent connection to traumatic events(panic attack) or arise in the immediacy–within a month–of trauma(acute stress disorder) or later(posttraumatic stress disorder),
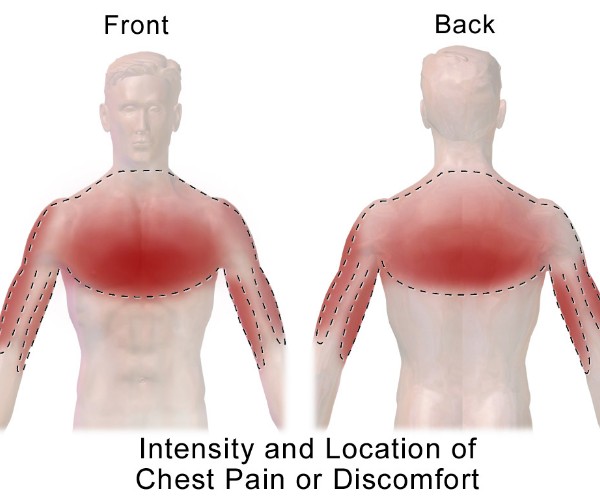
Anxiety may also present itself in clinical practice in the form of physical symptoms (somatization). Vegetative phenomena, sleep disturbances, asthenia, changes in appetite and sexuality, gastrointestinal complaints (e.g., abdominal cramps/pain), heaviness in the limbs, back, or head, back pain, muscle aches, and chest pain are examples of recurrent somatic symptoms during the course of an anxiety episode.
Many symptoms, such as asthenia, tremor, palpitations, easy fatigability, restlessness, insomnia, difficulty concentrating, feeling of lurching or unsteady balance, cephalalgic seizures, or other painful manifestations, are nonspecific and may conceal organic pathologies-thyroid dysfunction, neoplasms, myopathies, renal failure. Therefore, it is necessary to know how to diagnose them in a timely manner with the performance of specific laboratory or instrumental investigations, with the request for specialized consultations on the basis of suitable diagnostic hypotheses, after a careful assessment of the patient’s medical history, lifestyle and the context in which the disorder occurs.
It is not always possible to delineate a causal link between life events and the clinical picture; in some situations anxiety arises after a traumatic event or in conjunction with a period of particular stress, other times there are no apparent reasons for the onset of anxiety.
In fact, the pathogenesis is multifactorial. It is not easy to determine the responsiveness or otherwise of an anxiety disorder, even those that may seem to be disorders clearly related to life events may not be on closer examination; conversely, seemingly insignificant events for most people may have clear pathogenic significance in some circumstances
It is important in any case to consider the relationship of Anxiety Disorders to the subject’s personality.
Anxiety is ubiquitous, we find it in many medical and psychiatric conditions and it is present in daily life.
There is a wide area of symptom overlap between anxiety disorders and depression.
Fear, dread, worry, and anguish, pregnant experiences of the anxiety dimension, can coexist-with different tones and clinical modulations-with sadness, depressed mood, and experiences of guilt-characterizing the depressive dimension. It is essential to understand the reasons for the discomfort, the context and the ways in which it manifests itself, and what interventions can modify the discomfort, always remembering that behind the symptom is the person with his or her way of being and coping with life.
ANECDOTE
The fear of danger is ten thousand times more chilling than the danger itself: the weight of anxiety seems heavier to us than the evil feared. (Daniel Defoe)