When Enzo Maiorca, the father of freediving, who mastered its scenes in the 1970s together with J. Mayol, announced that he wanted to reach the depth of -50m, there was a French doctor, Cabarrou, who opposed such an attempt, justifying it on the grounds that, at that depth, the champion’s rib cage would implode.
He had simulated, in fact, the immersion of an average-sized man by getting a kind of wooden fruit box underwater, resembling, precisely, a human chest. At that altitude such an experimental contraption crumpled in on itself, hence the scholar’s concerns. The Italian champion, however, contravened medical orders by diving to the altitude he desired and emerged unharmed.
Thus began studies of the physiological transformations that occur in a human body when it approaches depth, and an extraordinary phenomenon was discovered to occur, which was given the name Blood Shift or pulmonary hemocompensation or pulmonary erection. It has been observed that this phenomenon is activated as soon as one begins to move in the water, together with the diving reflex, even in very few meters or centimeters even, of course it becomes of greater magnitude at deeper elevations. As we descend to the depths, the aerial parts of our body, by Boyle’s law, decrease in volume: at -40 meters the lung volume is 1/5 of what it is at the surface; at -100 meters it is 1/11 of the volume it is at sea level.
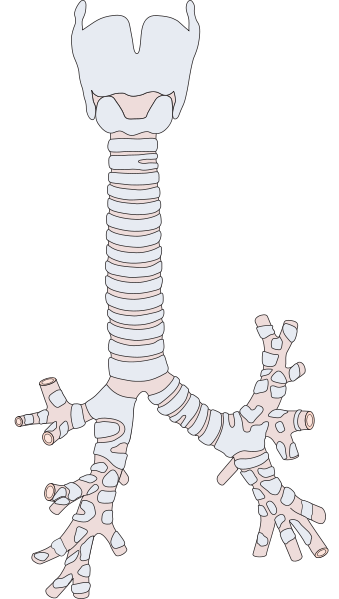
The space left empty inside the lungs, by air that, compressed, has shrunk in volume, if not occupied by anything would allow the rib cage to fold in on itself. And here intervenes not only the perfection of our bodies, designed to survive always and everywhere and yearning for such survival even in an extreme situation, but the genetic legacy that belongs to us anyway, of life that was born in water.
The rib cage begins to fill with blood, drawn from the peripheral areas. This serves two functions:
(a) blood is a fluid and, as such, is incompressible; therefore, it protects the chest from implosion;
(b) flowing out of the peripheral areas, legs and arms, will begin 1) to be sprayed and to be “defended” only the vital organs and furthermore, 2) the body, sensing that it is in an extreme and dangerous situation, tries, in this way, to conserve oxygen as much as possible, promoting the athlete’s apneas.





Such blood, moreover, is very thick and lacks the watery part, as a hormone is activated in the diver that induces a frequent urge to urinate. When performances become demanding, and we are talking about dives over 50 meters, the blood shift begins to take on important characteristics, so it is essential to observe serious and adequate recovery times.
As it resurfaces, in fact, the blood returns to the peripheral areas, but being denser, because it is deprived of the water it has expelled with peeing, it struggles and is slower to do so and must be given time to “reposition” itself in the right way. It is also advisable to drink a lot after apnea to replenish lost fluids, even where the need is not felt. There is also to be said that professional athletes use such breathing techniques (glossopharyngeal or carp breathing) that they store a huge amount of air, during the last breath before a performance, much larger than during a normal inhalation.






Such methods involve that, in ascent, the diver slows down a bit, since the lung volume, which is approaching its original size, no longer immediately finds all of its space, the space it had at the beginning, before the deep dive, since, part of it, may still be occupied by the blood that, slowly, flows out to the periphery of our body.
Sometimes it is necessary for such divers to “debouch” even a little before surfacing, otherwise, upon exiting their dive, they may detect some blood traces in their saliva, due to the rupture of capillaries present in the lungs, in which there is still a lot of blood and insufficient space to contain it along with the air, which regains an expansion of volume equal to that which characterized it at the start.
by Mariafelicia Carraturo
www.feliciacarraturo.it